Talk:Clobenzorex
| Summary sheet: Clobenzorex |
| Clobenzorex | |||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
 |
|||||||||||||||||||||||||||||||||||
| Chemical Nomenclature | |||||||||||||||||||||||||||||||||||
| Common names | Clobenzorex, Asenlix, Dinintel, Finedal, Rexigen, Itravil, Greenies | ||||||||||||||||||||||||||||||||||
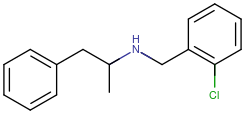
| Substitutive name | N-(2-Chlorobenzyl)amphetamine | ||||||||||||||||||||||||||||||||||
| Systematic name | ? | ||||||||||||||||||||||||||||||||||
| Class Membership | |||||||||||||||||||||||||||||||||||
| Psychoactive class | Stimulant | ||||||||||||||||||||||||||||||||||
| Chemical class | Amphetamine | ||||||||||||||||||||||||||||||||||
| Routes of Administration | |||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||
| Interactions | |||||||||||||||||||||||||||||||||||
Clobenzorex (also known under the brand names Asenlix, Finedal and Rexigen; or the US slang "greenies") is a novel stimulant substance of the amphetamine class. It is an N-alkyl-substituted amphetamine prodrug for d-amphetamine (dextroamphetamine) [2] used as an anorectic (a medication that suppresses appetite). The drug is legally distributed in Mexico as a part of a weight-management program.[3] Like amphetamine, clobenzorex produces its effects by promoting the release of neurotransmitters dopamine and norepinephrine in the brain. Its anorexigenic activity is produced by activating α- and β-adrenergic receptors in the lateral hypothalamus.[4][5]
Subjective effects are essentially identical to that of dextroamphetamine except with ? ? and a longer duration. These include stimulation (in a small percent of the population paradoxal sedation), focus enhancement, motivation enhancement, euphoria, and in a smaller population . ? lisdexamfetamine, clobenzorex was designed to prevent non-oral forms of administration. This means that sublingual, insufflation, smoking or injection do not provide faster absorption or onset. It had been used in the 1970s by US baseball players to reduce fatigue, increase attention and improve reaction times during athletic activities.
Despite being approximately one-twentieth the potency by weight of dextroamphetamine[6], many users report that clobenzorex is capable of producing dependence and addiction like other euphoric stimulants, particularly when it is taken above the recommended dosage. As a result, it is highly advised to use harm reduction practices if using this substance.
History and culture
This History and culture section is a stub. As a result, it may contain incomplete or wrong information. You can help by expanding it. |
Clobenzorex was developed by Aventis as a ? of dextroamphetamine.[7]
The ? approved clobenzorex for obesity treatment in adults on the DD[th/st] of [Month] YYYY [8], followed by an approval ? in adults in [Month] YYYY. [9]
Chemistry
Clobenzorex is a ? composed of the ?, ? ? bonded to dextroamphetamine.[10] Amphetamine is comprised of a phenethylamine core featuring a phenyl ring bound to an amino (NH2) group through an ethyl chain with an additional methyl substitution at Rα. It can be referred to as a methyl homologue of phenethylamine as it has the same general formula, differing only in the addition of one methyl group.
Pharmacology
Clobenzorex was developed with the goal of providing a ? that ? as well as ?. The attachment of the ? ? slows down the relative amount of dextroamphetamine that is ?. Because no free dextroamphetamine is present in clobenzorex capsules, dextroamphetamine does not become available through mechanical manipulation, such as crushing or simple extraction. There is, therefore, no way to speed up absorption via alternate routes of administration, such as via insufflation, vaporization, or injection, making the drug ?.
Pharmacokinetics
As a prodrug, clobenzorex is inactive in the form administered. Once ingested, it is enzymatically cleaved into two parts: 4-Hydroxyclobenzorex, a hydroxy ? , and dextroamphetamine, a central nervous system stimulant. Thus clobenzorex functions as a ? version of dextroamphetamine. Because dextroamphetamine needs to be liberated from 2'-chlorotoulene via contact with hepatic CYP3A4 and CYP2B6 isoenzymes, effects are independent of route of administration. Conversion of clobenzorex into active dextroamphetamine is enzymatically rate-limited, slowing down the time to achieve peak concentrations and decreasing its magnitude and dampening consequent striatal dopamine release, which is thought to be responsible for its euphoric and compulsive redosing effects.
Clobenzorex can be detected in urine, which can cause false positives for workplace drug screening.[11] It is one of many drugs that can cause false positives for amphetamine urine drug screening.[12] It may be differentiated from amphetamine use through testing for 4-hydroxyclobenzorex[13] or enantiomeric analysis.[14]
Pharmacodynamics
Amphetamine is a full agonist of the trace amine-associated receptor 1 (TAAR1), which is a key regulator of common and trace brain monoamines such as dopamine, serotonin and noradrenaline.[15][16][17] The agonism of this set of receptors results in the release of increased concentrations of dopamine, serotonin and noradrenaline in the synaptic cleft. This leads to cognitive and physical stimulation within the user.
Dextroamphetamine's affinity for the TAAR1 receptor is twice that of l-amphetamine.[18] As a result, dextroamphetamine produces three to four times as much central nervous system (CNS) stimulation as levoamphetamine. Levoamphetamine, on the other hand, has stronger cardiovascular and peripheral effects.
Conversion rate
15% of the weight of clobenzorex hydrochloride (the usual prescribed form) is dextroamphetamine: 30 mg clobenzorex hydrochloride is equivalent to 4.5 mg of dextroamphetamine.[19][20]
The subjective experience will differ due to the slower, more steady onset of active substance in the prodrug. An equivalent dose of dextroamphetamine will have a higher peak plasma concentration and shorter duration.
Subjective effects
While the subjective effects are almost identical to that of amphetamine, clobenzorex is significantly in its duration and more consistent in its intensity due to the ? metabolism to dextroamphetamine.
Peripheral effects (such as increased heart rate and higher body temperature) are reported to be less prominent than formulations that partly contain levoamphetamine, such as Adderall or the racemic amphetamine sulphate sold illicitly.
Disclaimer: The effects listed below cite the Subjective Effect Index (SEI), an open research literature based on anecdotal user reports and the personal analyses of PsychonautWiki contributors. As a result, they should be viewed with a healthy degree of skepticism.
It is also worth noting that these effects will not necessarily occur in a predictable or reliable manner, although higher doses are more liable to induce the full spectrum of effects. Likewise, adverse effects become increasingly likely with higher doses and may include addiction, severe injury, or death ☠.
Physical effects 
-
- Stimulation - Clobenzorex is reported to be very energetic and stimulating in a manner similar to lisdexamfetamine. It can encourage physical activities such as dancing, socializing, running, or cleaning. The particular style of stimulation which clobenzorex produces can be described as forced. This means that, at higher dosages, it becomes difficult or impossible to keep still as jaw clenching, involuntary bodily shakes and vibrations become present, resulting in extreme shaking of the entire body, unsteadiness of the hands, and a general loss of fine motor control. This effect is replaced with mild fatigue and general exhaustion during the offset of the experience.
- Spontaneous bodily sensations - The "body high" of clobenzorex can be described as a moderate euphoric tingling sensation that encompasses the entire body. This sensation maintains a consistent presence that steadily rises with the onset and hits its limit once the peak has been reached.
- Abnormal heartbeat
- Increased heart rate
- Increased blood pressure
- Appetite suppression - This effect is more pronounced compared to amphetamine, sometimes causing people to not eat for the entire duration of action. Clobenzorex is commonly prescribed to treat obesity due to its strong appetite suppressing effect.[21]
- Bronchodilation
- Muscle tension
- Dehydration
- Dry mouth
- Frequent urination
- Increased bodily temperature
- Increased perspiration
- Nausea - This effect usually only occurs at heavy doses.
- Pupil dilation - This effect is more prominent on the offset of the experience and usually only occurs at common to heavy doses.
- Stamina enhancement
- Teeth grinding - This component can be considered to be less intense when compared with that of MDMA.
- Temporary erectile dysfunction
- Vasoconstriction
Visual effects 
-
The visual effects of clobenzorex are usually less consistent and only mildly noticeable at higher dosages. They are somewhat comparable to the visual effects of deliriants and occur more readily in darker areas.
Enhancements
- Visual acuity enhancement
- Double vision - Amphetamines can cause double vision at high doses.
Distortions
- Drifting (breathing and morphing) - This effect is usually subtle and only occurs at higher doses, after long periods of being awake, or when combined with cannabis. Commonly this consists of level 1-2 drifting.
- Brightness alteration - Clobenzorex can make spaces seem brighter as a result of its pupil dilating effects.
Hallucinatory states
- Transformations - This effect occurs very rarely, and typically only when the user has taken high doses, is coming down, or has been awake for unusually long periods. They are usually very mild when they do occur.
Cognitive effects 
-
Clobenzorex shares most of its cognitive effects with other amphetamines, although it is less forceful in its come up due to the slower metabolism. It produces a variety of cognitive enhancements associated with stimulants. However, during the latter part of the duration, these cognitive enhancements may compete with or be nullified by the accumulated dopamine depletion and its effects.
The most prominent of these cognitive effects generally include:
- Analysis enhancement
- Anxiety - This effect occurs more frequently on the offset phase of the experience.
- Creativity enhancement
- Compulsive redosing - Due to the slow come up of clobenzorex, the full effects may not be felt for up to three hours after consumption, causing some to redose during the come up. Compulsive redosing is more common if heavy doses are taken.
- Ego inflation
- Emotion suppression
- Focus enhancement
- Irritability
- Immersion enhancement
- Increased music appreciation
- Memory enhancement
- Motivation enhancement
- Increased libido or Decreased libido
- Novelty enhancement
- Time distortion - This can be described as the experience of time speeding up and passing much quicker than it usually would when sober.
- Thought acceleration
- Thought organization
- Wakefulness
- Cognitive euphoria
Auditory effects 
-
- Enhancements
- Hallucinations - Use of clobenzorex and other amphetamines, at a strong or heavy dose, can occasionally cause mild auditory hallucinations. These hallucinations most commonly occur amongst a source of white noise, such as a fan, and typically consist of quiet phantom music or voices. Clobenzorex may also cause auditory hallucinations in the form of stimulant psychosis.
After effects 
- The effects which occur during the offset of a stimulant experience generally feel negative and uncomfortable in comparison to the effects which occurred during its peak. This is often referred to as a "comedown" and occurs because of neurotransmitter depletion. The comedown produced by clobenzorex is often reported to be much less intense than its metabolite, dextroamphetamine, due to its ?. Its effects commonly include: Making sure to eat well and to hydrate are recommended to decrease the severity of comedown effects. Using mild sedatives is also a common strategy for stimulant comedowns.
Experience reports
There are currently 0 experience reports which describe the effects of this substance in our experience index.
Toxicity and harm potential
In rodents and primates, sufficiently high doses of amphetamine cause dopaminergic neurotoxicity, or damage to dopamine neurons, which is characterized by reduced transporter and receptor function. There is no evidence that amphetamine is directly neurotoxic in humans. However, large doses of amphetamine may cause indirect neurotoxicity as a result of increased oxidative stress from reactive oxygen species and autoxidation of dopamine.
It is strongly recommended that one use harm reduction practices when using this drug.
Tolerance and addiction potential
Addiction is a serious risk with heavy recreational amphetamine use but is unlikely to arise from typical long-term medical use at therapeutic doses. Clobenzorex has been posited to have less potential for abuse and addiction than other pharmaceutical amphetamines due to the slower onset and the reduced potency, which puts a cap on the maximum peak plasma concentration and consequent dopamine release. Caution is nonetheless advised, as with other drugs in the amphetamine class.
Tolerance develops rapidly in amphetamine abuse (i.e. a recreational amphetamine overdose), so periods of extended use require increasingly larger doses of the drug in order to achieve the same effect. Repeated use of clobenzorex will result in a gradual tolerance proportional to the dosage taken. Patients prescribed this drug often must increase their dosage after a time to maintain its efficacy.
Overdose
A severe amphetamine overdose can result in a stimulant psychosis that may involve a variety of symptoms, such as paranoia, delusions, and hallucinations, including the infamous Shadow people. A Cochrane Collaboration review on treatment for amphetamine, dextroamphetamine, and methamphetamine psychosis states that about 5–15% of users fail to recover completely. According to the same review, there is at least one trial that shows antipsychotic medications effectively resolve the symptoms of acute amphetamine psychosis. Psychosis very rarely arises from therapeutic use. The combination of prolonged use of high doses combined with sleep deprivation significantly increases the risk of stimulant psychosis.
Dangerous interactions
Warning: Many psychoactive substances that are reasonably safe to use on their own can suddenly become dangerous and even life-threatening when combined with certain other substances. The following list provides some known dangerous interactions (although it is not guaranteed to include all of them).
Always conduct independent research (e.g. Google, DuckDuckGo, PubMed) to ensure that a combination of two or more substances is safe to consume. Some of the listed interactions have been sourced from TripSit.
- Alcohol - Drinking alcohol on stimulants is considered risky because it reduces the sedative effects of the alcohol that the body uses to gauge drunkenness. This often leads to excessive drinking with greatly reduced inhibitions, increasing the risk of liver damage and increased dehydration. The effects of stimulants will also allow one to drink past a point where they might normally pass out, increasing the risk. If you do decide to do this then you should set a limit of how much you will drink each hour and stick to it, bearing in mind that you will feel the alcohol and the stimulant less.
- GHB/GBL - Stimulants increase respiration rate allowing a higher dose of sedatives. If the stimulant wears off first then the depressant effects of the GHB/GBL may overcome the user and cause respiratory arrest.
- Opioids - Stimulants increase respiration rate allowing a higher dose of opiates. If the stimulant wears off first then the opiate may overcome the patient and cause respiratory arrest.
- Cocaine - The rewarding effects of cocaine are mediated by DAT inhibition, and an increase of exocytosis of dopamine through the cell membrane. Amphetamine reverses the direction of DAT and the direction vesicular transports within the cell by a pH mediated mechanism of displacement, thus excludes the regular mechanism of dopamine release through means of exocytosis because the effects Na+/K+ ATPase are inhibited. You will find cardiac effects with the combination of cocaine and amphetamine due to a SERT mediated mechanism from the subsequent activation of 5-HT2B, which is an effect of serotonin-related valvulopathy. Amphetamines generally cause hypertension in models of abuse, and this combination can increase the chances of syncope due to turbulent blood flow during valve operation. The rewarding mechanisms of cocaine are reversed by administration of amphetamine.[22][23]
- Cannabis - Stimulants increase anxiety levels and the risk of thought loops and paranoia which can lead to negative experiences.
- Caffeine - This combination of stimulants is generally considered unnecessary and may increase strain on the heart, as well as potentially causing anxiety and physical discomfort.
- Tramadol - Tramadol and stimulants both increase the risk of seizures.
- DXM - Both substances raise heart rate, in extreme cases, panic attacks caused by these substances have led to more serious heart issues.
- Ketamine - Combining amphetamine and ketamine may result in psychoses that resemble schizophrenia, but not worse than the psychoses produced by either substance alone, but this is debatable. This is due to amphetamines ability to attenuated the disruption of working memory caused by ketamine. Amphetamine alone may result in grandiosity, paranoia, or somatic delusions with little to no effect on negative symptoms. Ketamine, however, will result in thought disorders, disruption of executive functioning, and delusions due to a modification of conception. These mechanisms are due to an increase of dopaminergic activity in the mesolimbic pathway caused by amphetamine due to its pharmacology effecting dopamine, and due to a disruption of dopaminergic functioning in the mesocortical pathways via NMDA antagonism effects of ketamine. Combining the two, you may expect mainly thought disorder along with positive symptoms.[24]
- PCP - Increases risk of tachycardia, hypertension, and manic states.
- Methoxetamine - Increases risk of tachycardia, hypertension, and manic states.
- Psychedelics (e.g. LSD, mescaline, psilocybin) - Increases risk of anxiety, paranoia, and thought loops.
- 25x-NBOMe - Amphetamines and NBOMes both provide considerable stimulation that when combined they can result in tachycardia, hypertension, vasoconstriction and, in extreme cases, heart failure. The anxiogenic and focusing effects of stimulants are also not good in combination with psychedelics as they can lead to unpleasant thought loops. NBOMes are known to cause seizures and stimulants can increase this risk.
- 2C-T-x - Suspected of mild MAOI properties. May increase the risk of hypertensive crisis.
- 5-MeO-xxT - Suspected of mild MAOI properties. May increase the risk of hypertensive crisis.
- DOx
- aMT - aMT has MAOI properties which may interact unfavorably with amphetamines.
- MAOIs - MAO-B inhibitors can increase the potency and duration of phenethylamines unpredictably. MAO-A inhibitors with amphetamine can lead to hypertensive crises.
Legal status
Clobenzorex is ?, but in most countries it is ?.
It is banned by the World Anti-Doping Agency for use during sports competitions.[25]
- Brazil: Clobenzorex is a Class A3 controlled prohibited psychotropic.[26]
- Canada: Clobenzorex is not specifically listed in the CDSA, however due to structural similarities with norbenzphetamine, it is a Schedule I under item 19(17).[citation needed]
- United Kingdom: Clobenzorex is a Class B controlled drug.[27]
- United States: Clobenzorex is not scheduled and is unaffected by the Federal Analogue Act as a derivative of Benzphetamine.[28]
Author, A. (Y ear). Title [Media Type]. Source. URL
Importation for personal use is lawful provided that is for use to treat a condition with no approved medications, unlawful marketing is not occurring in the U.S, not deemed hazardous to health for the treating the condition, and is verified as a continuation of a treatment plan that began in a foreign country.[29]
See also
External links
Literature
- Young, R., Darmani, N. A., Elder, E. L., Dumas, D., & Glennon, R. A. (1997). Clobenzorex: Evidence for amphetamine-like behavioral actions. Pharmacology, Biochemistry, and Behavior, 56(2), 311–316. https://doi.org/10.1016/S0091-3057(96)00329-2
- Cody, J. T. & Valtier, S. (2001). Amphetamine, clobenzorex, and 4-hydroxyclobenzorex levels following multidose administration of clobenzorex. Journal of Analytical Toxicology, 25(3), 158–165. https://doi.org/10.1093/jat/25.3.158
References
- ↑ Last, A. A., Last, B. B., ..., & Last, Z. Z. (YYYY). "?". ?. # (#): #–#. doi:? Check
|doi=value (help). - ↑ Cody, J. T. (2005). "Amphetamines: Methods of forensic analysis". In F P Smith & S A Athanaselis (Eds.). [google.com/books/edition/Handbook_of_Forensic_Drug_Analysis/8JsQgRO3QcwC?hl=en&gbpv=1&dq=Clobenzorex+metabolism&pg=PA430&printsec=frontcover Handbook of forensic drug analysis] Check
|url=value (help) (1st ed.). Elsevier. pp. 357–451. Vancouver style error: punctuation (help) - ↑ Young, R., Darmani, N. A., Elder, E. L., Dumas, D., & Glennon, R. A. (1997). "Clobenzorex: Evidence for amphetamine-like behavioral actions". Pharmacology, Biochemistry, and Behavior. 56 (2): 311–316. doi:10.1016/s0091-3057(96)00329-2.
- ↑ Argüelles-Tello, F., Carrasco-Portugal, M. del C., Carrasco-Portugal, N. A., Aguilar-Carrasco, J. C., Patiño-Camacho, S. I., del Valle, C. F., Reyes-Garcia, G., & Flores-Murrieta, F. J. (2013). "Comparison on the pharmacokinetics and weight reduction of clobenzorex slow release and immediate release formulations in obese patients". Pharmacology & Pharmacy. 4 (2): 218–221. doi:10.4236/pp.2013.42030.
- ↑ Cortés-Moreno, G. Y., Adrian, H.-H., Ángel, M.-G., Raúl, M.-Z., Rafael, G.-D., & Eleazar, L.-P. (2017). "Possible peripheral lipolytic effect of clobenzorex hydrochloride in patients with obesity". Medico Research Chronicles. 4 (3): 252–265.
- ↑ Young, R., Darmani, N. A., Elder, E. L., Dumas, D., & Glennon, R. A. (1997). "Clobenzorex: Evidence for amphetamine-like behavioral actions". Pharmacology, Biochemistry, and Behavior. 56 (2): 311–316. doi:10.1016/s0091-3057(96)00329-2.
- ↑ Last N, A A & Last Name, B B (YYYY). "Untitled". Untitled. ## (#): #–#. doi:10.????/S????????????????. PMID ???????? Check
|pmid=value (help). Vancouver style error: initials (help) - ↑ [http:example.com/untitled/document.pdf "Untitled"] (PDF). example.com. Retrieved DD [Month] YYYY.
- ↑ "Untitled". Untitled (Press release). DD [Month] YYYY. Retrieved DD [Month] YYYY. Unknown parameter
|url-status=ignored (help);|archive-url=is malformed: timestamp (help) - ↑ ? (YYYY). [? "?"] Check
|url=value (help). ?. # (#): #–#; discussion #–#. doi:10.????/?. PMID ? Check|pmid=value (help). Vancouver style error: non-Latin character (help) - ↑ ?
- ↑ ?
- ↑ Cody, J. T., & Valtier, S. (2001). "Amphetamine, clobenzorex, and 4-hydroxyclobenzorex levels following multidose administration of clobenzorex". Journal of Analytical Toxicology. 25 (3): 158–165. doi:10.1093/jat/25.3.158.
- ↑ ?
- ↑ Miller, G. M. (2011). "The emerging role of trace amine-associated receptor 1 in the functional regulation of monoamine transporters and dopaminergic activity". Journal of Neurochemistry. 116 (2): 164–176. doi:10.1111/j.1471-4159.2010.07109.x.
- ↑ Drug banks amphetamine targets
- ↑ TA1 receptor |http://www.iuphar-db.org/DATABASE/ObjectDisplayForward?objectId=364
- ↑ Lewin, A. H., Miller, G. M., & Gilmour, B. (2011). "Trace amine-associated receptor 1 is a stereoselective binding site for compounds in the amphetamine class". Bioorganic & Medicinal Chemistry. 19 (23): 7044–7048. doi:10.1016/j.bmc.2011.10.007.
- ↑ https://www.medicamentosplm.com/Home/productos/asenlix.capsulas/160/101/77500/14#rubro-2
- ↑ ?
- ↑ ?
- ↑ Greenwald, M. K., Lundahl, L. H., Steinmiller, C. L. (December 2010). "Sustained Release d-Amphetamine Reduces Cocaine but not 'Speedball'-Seeking in Buprenorphine-Maintained Volunteers: A Test of Dual-Agonist Pharmacotherapy for Cocaine/Heroin Polydrug Abusers". Neuropsychopharmacology. 35 (13): 2624–2637. doi:10.1038/npp.2010.175. ISSN 0893-133X.
- ↑ Siciliano, C. A., Saha, K., Calipari, E. S., Fordahl, S. C., Chen, R., Khoshbouei, H., Jones, S. R. (10 January 2018). "Amphetamine Reverses Escalated Cocaine Intake via Restoration of Dopamine Transporter Conformation". The Journal of Neuroscience. 38 (2): 484–497. doi:10.1523/JNEUROSCI.2604-17.2017. ISSN 0270-6474.
- ↑ Krystal, J. H., Perry, E. B., Gueorguieva, R., Belger, A., Madonick, S. H., Abi-Dargham, A., Cooper, T. B., MacDougall, L., Abi-Saab, W., D’Souza, D. C. (1 September 2005). "Comparative and Interactive Human Psychopharmacologic Effects of Ketamine and Amphetamine: Implications for Glutamatergic and Dopaminergic Model Psychoses and Cognitive Function". Archives of General Psychiatry. 62 (9): 985. doi:10.1001/archpsyc.62.9.985. ISSN 0003-990X.
- ↑ (n.d.) (2022). "World anti-doping code international standard prohibited list 2023" (PDF). World Anti-Doping Agency.
- ↑ Anvisa (2023-07-24). "RDC Nº 804 - Listas de Substâncias Entorpecentes, Psicotrópicas, Precursoras e Outras sob Controle Especial" [Collegiate Board Resolution No. 804 - Lists of Narcotic, Psychotropic, Precursor, and Other Substances under Special Control] (in Portuguese). Diário Oficial da União (published 2023-07-25). Archived from the original on 2023-08-27. Retrieved 2023-09-28.
- ↑ "Misuse of Drugs Act 1971 (c. 38): SCHEDULE 2: Controlled Drugs". Office of Public Sector Information. Retrieved 2009-06-15.
- ↑ (Boos, T.) (2023). "Clobenzorex letter". Imgur (Image). Archived from the original
|archive-url=requires|url=(help) on|archive-url=requires|archive-date=(help). - ↑ (n.d.) (2021). "Is it legal for me to personally import drugs?". Food and Drug Administration.